Case management is a social work model for the provision of protection and assistance to individuals with complex and multiple needs who require access to a variety of services. MRRMs’ protection and assistance services follow a migrant-centered (or client-oriented) approach to case management, ensuring that the interest of each individual is at the center of all interventions. This approach also promotes beneficiaries’ participation and decision-making regarding their access to MRRMs’ services.
Case management allows to address beneficiaries’ needs in an appropriate, systematic, and timely manner either through direct assistance or referrals. In order to ensure quality, consistency, and coordination of assistance, case management shall be provided in accordance with standard operating procedures (SOPs) to be established for each centre in line with its components and objectives.
Depending on the migratory context and on the safety and security of both migrants and caseworkers, different delivery models can be put in place or combined to provide the best possible assistance. In the individual care model, individual caseworkers are assigned to beneficiaries on a one-to-one basis. This model allows us to build trust between the two subjects but is highly resource-intensive. In the community-based care model, case managers are based in migrant communities, allowing for more direct access to the targeted population and enhanced knowledge of available services among the beneficiaries. Outreach/mobile models foresee that caseworkers meet beneficiaries in their place of residence, accommodation, or in other convenient locations, and it is recommended when beneficiaries do not want to or cannot be identified by going to an migrant centre. Caseworkers are usually based in migrant centres facilities, but remote case management via phone or internet is also possible.
Case management is not a linear process but it may be divided into six interlinked steps :
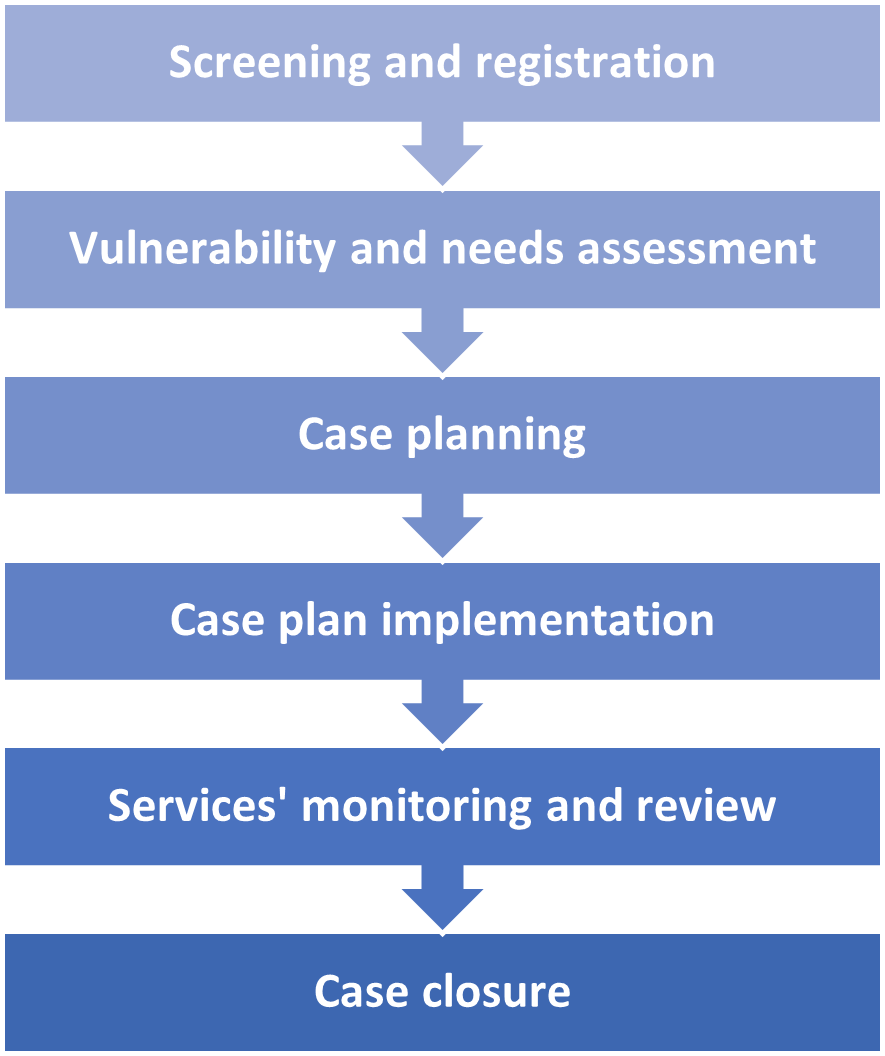
a) Screening and registration: Eligibility criteria to access MRRMs’ protection and assistance services shall be clearly defined prior to programme implementation in order to guide the screening process that will lead to beneficiaries’ admission. Registration starts once caseworkers have verified that eligibility criteria are met and the beneficiary has given informed consent to registration. Registration of beneficiaries accessing migrant centres allows to ensure current individual and future case management, to monitor assistance delivery, to identify gaps and needs and to avoid duplication of services and fraud. Data can be collected both at individual and household level and it usually includes disaggregated demographic information such as names, date of birth, sex, gender, as well as other elements including vulnerabilities, reasons for migrating and experiences of hardship and abuses. For more detailed guidance on registration of beneficiaries, please consult this entry.
b) Vulnerability and needs assessment: Once an individual is identified as eligible for assistance, a comprehensive assessment shall be made to determine their vulnerability and needs. Vulnerability screenings consist in the identification and assessment of situations of vulnerability, including for instance medical and psychological needs, unaccompanied and separated migrant children, victims of trafficking, exploitation, abuse, gender violence or gender discrimination, as well as persons in need of international protection. IOM’s determinants of migrant vulnerability (DoMV) model has been developed to identify, protect and assist migrants who have experienced or are vulnerable to violence, exploitation and abuse and to guide the development and implementation of interventions to reduce vulnerability. The model encompasses both risk and protective factors and can be applied before, during or after migration. The DoMV model provides practitioners with an operational methodology and practical tools for understanding and assessing the factors that determine migrant vulnerability taking into account a) individual factors, as for instance age, sex, racial and/or ethnic identity, sexual orientation, gender identity, personal history, mental health and psychosocial wellbeing, and access to resources; b) household and family factors such as family size, household structure, socioeconomic status, migration histories, employment, livelihoods, education levels, gender discrimination and family dynamics; c) community factors including availability of quality educational opportunities, health care and social services, as well as access to resources and livelihood opportunities and d) structural factors concerning the political, economic, social and environmental conditions.
c) Case planning: Individual case plans address the needs identified during the assessment phase by identifying measurables objectives to be reached through direct assistance and/or referrals. Beneficiaries shall play an active role in the elaboration of their plan, working closely with their designated caseworker to ensure that their goals, needs and priorities stand out. Case plans shall be detailed and define the actions shall be taken, who is responsible for their implementation and within what time framework. The documents shall specify how assistance will be monitored, how feedback from beneficiaries will be incorporated and how information will be shared with beneficiaries and between caseworkers and relevant counterparts. The plans can also include resource allocations and a budget for relevant costs. They are living documents that can be revised if the situation or the context change, and they shall address beneficiaries’ needs in the short, medium and long term.
d) Case plan implementation: This step concerns the actions taken to implement the case plan through protection and assistance services, either through direct support by IOM or through referrals to other entities or implementing partners. In this phase, the caseworker has the responsibility to coordinate the provision of services and to monitor it, to record progress, and to make sure that case plan objectives are met. For an overview of MRRMs’ main protection and assistance services, please consult the entries in this category.
e) Services’ monitoring and review: Throughout the implementation of the assistance plan, caseworkers shall monitor the services accessed by beneficiaries to ensure that the plan meets their needs and that they are receiving appropriate support. Monitoring should be regular, although its frequency depends on the situation of each beneficiary and their specific needs and vulnerability. If a need for adjustments emerges, any change shall be made through regular communication with the beneficiary and information-sharing with all relevant partners. Monitoring and review can be addressed during case planning meetings – i.e. meetings between the beneficiary and their caseworker; case management meetings – i.e. internal meetings to review open cases and to discuss about progresses and to discuss possible measures to be taken; and case conferences – i.e. meetings among all partners involved in the provision of assistance and services to a given beneficiary.
f) Case closure is the point at which assistance ends. Case management may terminate for a variety of reasons, as for instance because the support has ended, because beneficiaries no longer meet the criteria for case management support, because they choose to stop receiving assistance, or because they leave the location where assistance was provided. Before case closure, the beneficiary shall be prepared for the transition and any unmet or new needs identified. In MRRM programming, often cases are not closed but transferred to another IOM office (e.g. from a facility in a sub-office to a main office, or from an MRRM program to an IOM office in a country of destination or return). In this case, a clear handover plan shall be shared with the caseworker taking over the file. When transferring a case to a partner (e.g. to the government or to another UN agency), beneficiaries shall give informed consent.